
By Ibogaine By David Dardashti
The opioid crisis has mutated. Ten years ago, addiction medicine was primarily fighting heroin and prescription painkillers—substances with predictable half-lives and well-understood metabolic pathways. Today, the enemy is Fentanyl.
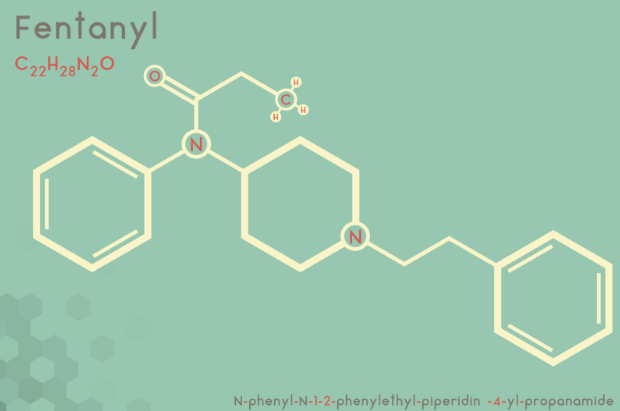
Fentanyl is not just “stronger heroin.” It is chemically distinct, highly lipophilic (fat-soluble), and often adulterated with other sedatives like Xylazine or benzodiazepines. Traditional “standardized” detox protocols are failing at alarming rates because they are trying to treat a 2025 problem with 1990s methodology.
To defeat Fentanyl, we cannot rely on guesswork or static dosing. We must rely on data. At Ibogaine by David Dardashti, we have developed an optimized treatment algorithm that applies the mathematical concept of implicit differentiation to the biological chaos of addiction. This isn’t just a detox; it is precision medicine.
The Pharmacokinetic Challenge of Fentanyl
To understand why an algorithm is necessary, one must first understand why Fentanyl is so difficult to treat.
Getty Images
Unlike heroin, which is water-soluble and leaves the body relatively quickly, Fentanyl binds to fat cells. It lingers in the body’s adipose tissue, slowly leaching back into the bloodstream days after the last use. This creates a “stuttering” withdrawal process. If a patient is treated with a standard dose of Ibogaine too early, they risk “precipitated withdrawal”—a state of intense physical agony caused by the medicine stripping opioids from the receptors before the bloodstream is clear.
Furthermore, street Fentanyl is rarely pure. It is a cocktail of analogues with varying potencies. A standard medical approach that assumes “One Size Fits All” is not only ineffective; it is dangerous.
The Solution: A Dynamic Algorithm
Our facility has moved away from static protocols. Instead, we have developed a proprietary algorithm that constructs a dosing strategy based on the individual’s unique history.
As David Dardashti explains, “By utilizing implicit differentiation, our algorithm is tailored specifically to the needs of each patient. This method allows us to adjust the algorithm based on the observations of previous operations, while taking into consideration the other substances the patient may be taking.”
In calculus, implicit differentiation is a technique used to find the rate of change when variables are dependent on one another in complex ways. In our medical context, it means we do not view “Fentanyl dosage” as a single, isolated number. We view it as a variable that changes relative to:
- Metabolic Rate (CYP2D6 enzyme activity): How fast the liver processes drugs.
- Adipose Storage: The patient’s Body Mass Index (BMI), which predicts how much Fentanyl is stored in fat.
- Potency History: The specific analogues the patient has been consuming.
By treating these as dependent variables, our software calculates a treatment trajectory that is unique to the patient’s physiology.
Addressing the “Polydrug” Interaction
One of the most critical aspects of our algorithm is its ability to account for drug interactions proactively.
The modern Fentanyl supply is frequently cut with Xylazine (a veterinary tranquilizer) or novel benzodiazepines. These substances affect the GABA receptors, while opioids affect the Mu-opioid receptors. A treatment that addresses only the opiates will leave the patient in severe seizure-risk withdrawal from the sedatives.
Our algorithm inputs these “co-occurring substances” as variables. If a patient tests positive for benzodiazepines or reports Xylazine use, the algorithm automatically adjusts the stabilization period. It calculates the necessary accumulation of Noribogaine (the long-acting metabolite of Ibogaine) required to soothe the nervous system without causing adverse interactions.
This proactive calculation minimizes the “shock” to the central nervous system, drastically reducing the physical and psychological side effects that usually terrify patients into avoiding treatment.
The “Time” Variable: Why We Added Days
A major output of our algorithmic analysis was the discovery that Fentanyl patients require a different timeline than heroin patients.
The algorithm frequently dictates additional days of treatment for those who are currently taking or have recently taken Fentanyl. This is not arbitrary; it is based on the calculated “washout” curve.
Shutterstock
Because Fentanyl stores in fat, the algorithm may suggest a Cumulative Micro-dosing Strategy leading up to a flood dose, rather than a single large dose on Day 1. This allows the Noribogaine to build up in the system, effectively “coating” the receptors and protecting them as the Fentanyl slowly leaves the fat cells.
- Traditional Method: Detox in 5 days. (High failure rate with Fentanyl).
- Algorithmic Method: The software might prescribe a 10-14 day protocol with specific booster treatments scheduled for Day 3, Day 5, and Day 8, based on the patient’s estimated clearance rate.
A Learning System
Perhaps the most revolutionary aspect of this approach is that it is iterative. The algorithm is “designed to account for any potential future opiate use, and any associated potency, by using the same core components but adjusting one variable at a time.”
Every patient treated contributes data points (anonymously) to the system. If the algorithm notes that patients with a specific BMI and usage history respond better to a slightly higher initial saturation dose, the model refines itself. We are effectively “adjusting based on the observations of previous operations,” creating a treatment protocol that gets smarter with every life saved.
Reducing Accessibility and Dependence
The ultimate goal of this technology is to “drastically reduce the accessibility of and dependence on fentanyl.” By making the detox process smoother, safer, and statistically more successful, we remove the primary barrier to recovery: Fear of Withdrawal.
Many addicts want to quit but are terrified of the pain. By using math to mitigate that pain—by calculating the precise window where treatment can occur without suffering—we are opening a door that was previously locked.
Conclusion: The Future is Data-Driven
We are standing on the precipice of a new era in addiction treatment. The days of “toughing it out” or using generic medical protocols are over. Fentanyl is a complex chemical adversary, and it requires a complex, calculated solution.
At Ibogaine by David Dardashti, we believe that the integration of implicit differentiation into medical protocols will revolutionize drug treatment around the world. We are not just treating addiction; we are solving it, one variable at a time.
For more information on our optimized algorithm and safety protocols, or to assess your own eligibility for treatment, please visit www.ibogaineclinic.com/ibogaine-treatment