

In urgent care, speed tends to get the most attention. Operators talk about patient throughput, registration efficiency, staffing flexibility, and the daily challenge of moving people through a high-volume outpatient setting without sacrificing quality of care. Yet one of the more important operational questions in urgent care is not simply how quickly a room can be turned. It is how consistently turnover happens from room to room, shift to shift, and team member to team member. In Baton Rouge, where outpatient demand continues to put pressure on clinics and urgent care centers, consistency in infection control is becoming a more serious issue for facilities. It is no longer enough for a site to say rooms are cleaned between patients. The stronger question is whether they are cleaned the same way every time, with the same touchpoints, in the same sequence, and with the same level of accountability.
Why Consistency Matters More Than Simple Room Turnover
Urgent care environments are built around repetition. The same types of interactions occur again and again throughout the day. Patients move in and out rapidly. Staff members multitask. Clinical teams are focused on care delivery, charting, and patient communication. In that setting, room cleaning can easily become a routine task that is not always managed as a standardized process. That distinction matters. A routine can be familiar yet vary in execution. A standardized process reduces variation. From an infection-control standpoint, that difference has real consequences because outpatient rooms contain high-touch surfaces, shared patient-contact areas, and repeated opportunities for small omissions that accumulate over time.
The practical problem is not always negligence. More often, it is an inconsistency created by operational pressure. One staff member may wipe the obvious surfaces but miss a secondary touchpoint. Another may change the sequence depending on how quickly the next patient is waiting. Another may assume that a surface cleaned earlier in the shift is still acceptable. Over the course of a busy day, these small differences can create a workflow that appears functional on the surface while drifting away from true consistency. In urgent care, where patient turnover is fast, and rooms may be used repeatedly within short windows, that drift can become one of the more important hidden risks in the facility environment.
Outpatient Standards Are Raising the Bar
Healthcare cleaning guidance has consistently emphasized the importance of repeatable procedures in patient care spaces. The CDC’s guidance on cleaning procedures in healthcare settings emphasizes systematic workflows, attention to high-touch surfaces, and consistent execution as part of infection-prevention practice. That framing is important because it shifts the conversation away from cleaning as a general housekeeping function and toward it as a controlled operational process. In urgent care, that means exam-room turnover should not be evaluated only by whether it was completed quickly. It should also be evaluated by whether it was completed correctly, thoroughly, and in a repeatable manner that does not depend too heavily on the habits of a single individual.
That expectation is especially relevant in outpatient care because these facilities are designed to balance accessibility with efficiency. Patients expect fast service, but they also expect visible cleanliness and quiet confidence in the environment around them. Those expectations overlap more than many operators realize. A room that looks clean may still reflect a weak process if critical touchpoints are not consistently addressed. Conversely, a well-structured cleaning workflow tends to support both patient trust and internal discipline. It gives staff members a defined sequence, reduces ambiguity, and creates a more defensible standard when managers need to train, audit, or correct performance.
Why Baton Rouge Is a Relevant Local Case
Baton Rouge provides a useful lens for this issue because it is both a local healthcare market and a growing outpatient environment. The region’s healthcare footprint continues to expand through urgent care, specialty clinics, and broader ambulatory services, which increases the importance of operational systems that can withstand daily volume. As more patient encounters move through outpatient settings, the room turnover process becomes more than a back-of-house task. It becomes part of the facility’s core ability to maintain order, continuity, and infection-control discipline while handling fluctuating demand.
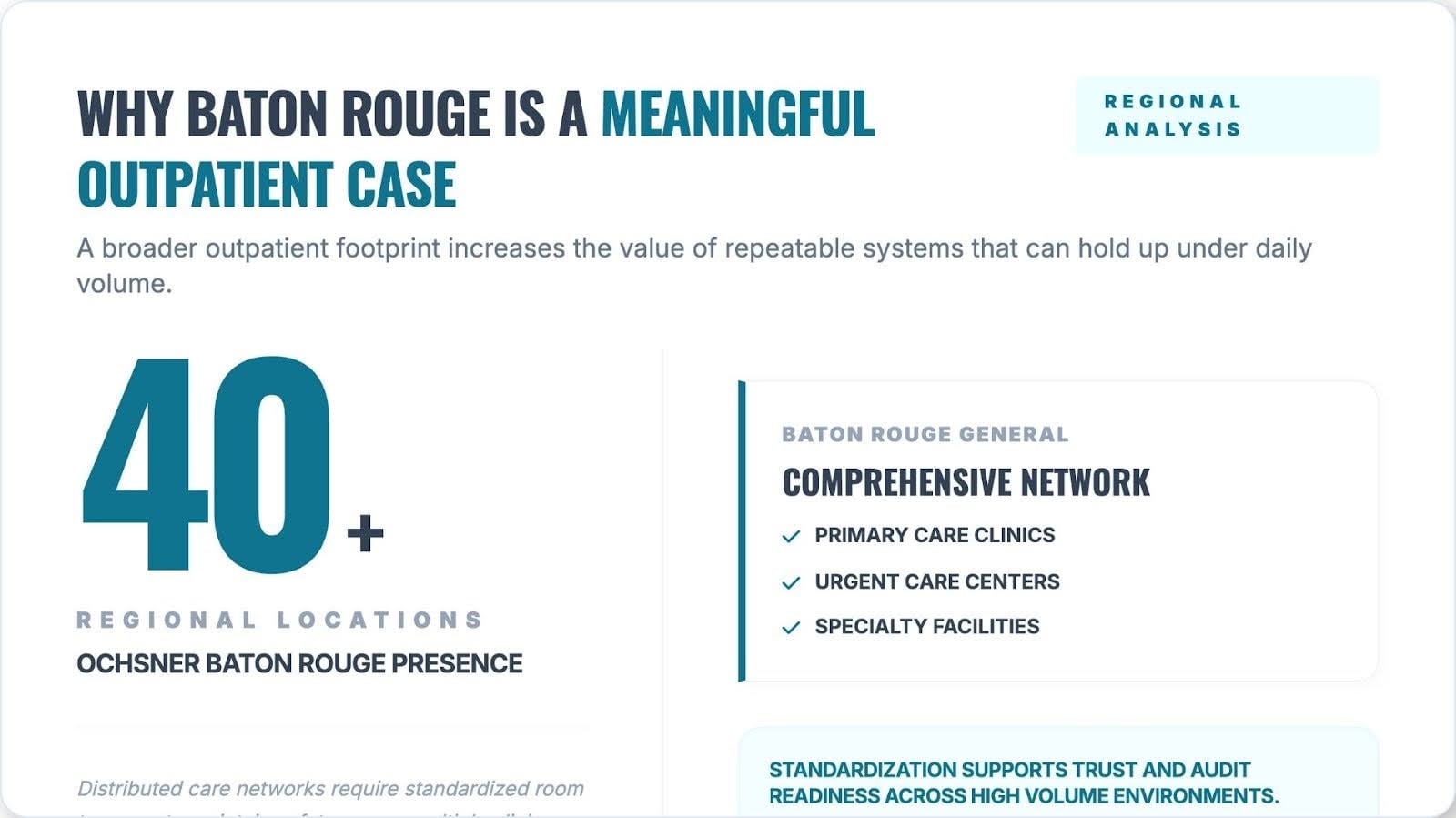
That is one reason local operators are paying closer attention to consistency rather than just frequency. A clinic may already understand that rooms need to be cleaned between patients. The harder question is whether the cleaning method is structured enough to produce the same result during a calm hour and during a surge period. In Baton Rouge, where urgent care centers often manage unpredictable patient flow across respiratory complaints, minor injuries, routine illnesses, and walk-in demand, workflow discipline matters. The exam room is not a neutral backdrop. It is a frequently used clinical environment where operational shortcuts can become habits if not actively controlled.
What a Standardized Exam-Room Workflow Looks Like
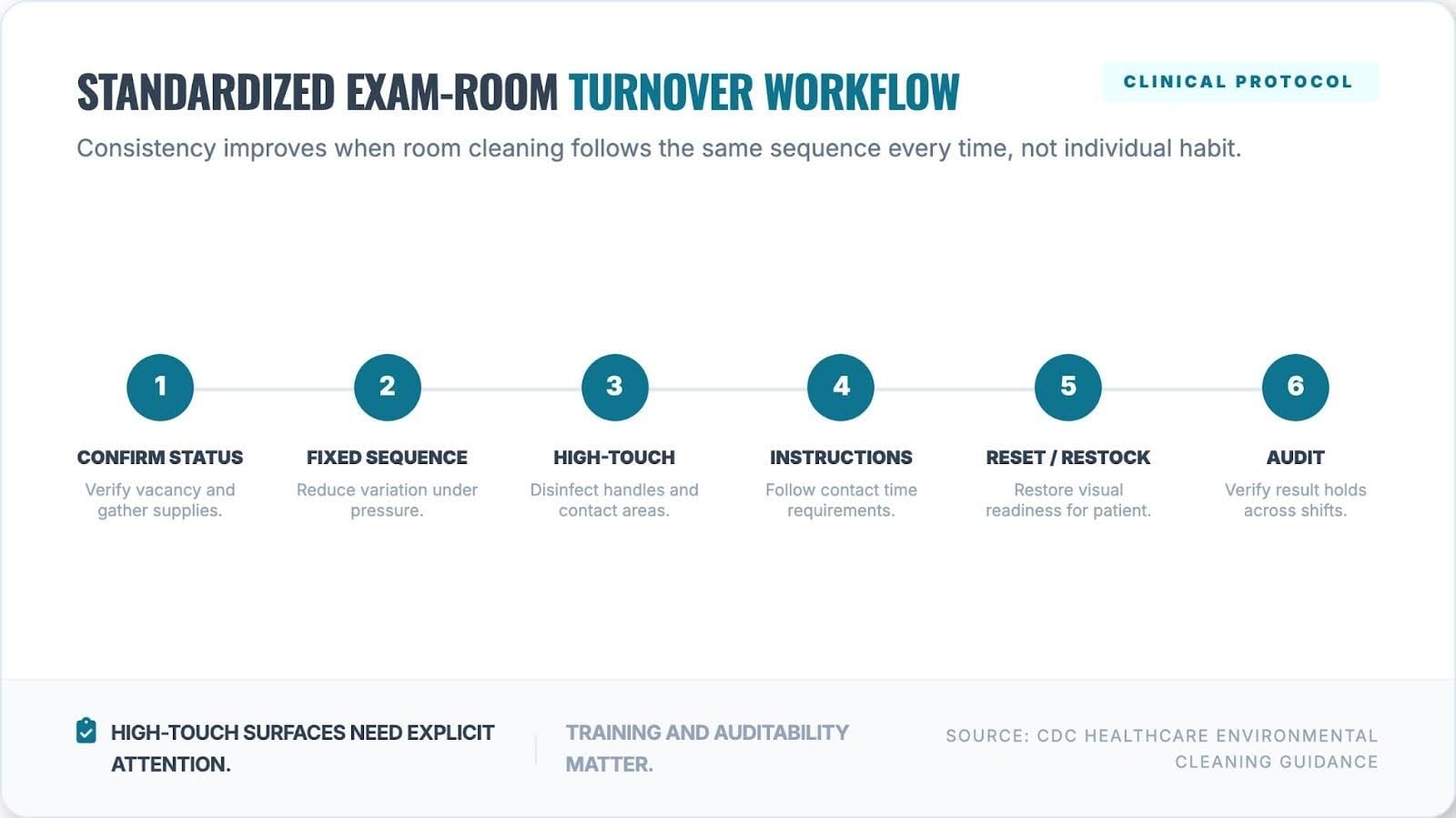
The strongest urgent care cleaning systems tend to be built around simple, repeatable steps rather than vague expectations. Staff members need to know exactly what is addressed, in what order, with which products, and to what visual standard for completion. That is why many facility leaders are moving toward more explicit room-turnover routines that reduce guesswork. The goal is not to slow the clinic down. It is to create a process that remains dependable even when the clinic is moving quickly.
A practical example of that approach appears in this exam-room cleaning workflow for urgent care facilities, which breaks the turnover process into a more structured sequence of operations. What makes that framework relevant is not just the cleaning itself, but the logic behind it. It treats the room as a system of repeated touchpoints rather than a generic space that needs to look tidy. In high-volume outpatient settings, that distinction is important because visual neatness and true process consistency are not the same thing. A workflow that identifies room status, surface priorities, and the order of tasks is more likely to support infection-control consistency than one that relies on memory or informal habits.
Why Clay Vavasseur Says Process Discipline Matters
Clay Vavasseur, owner of Advanced Office Care, points to consistency as the main operational divide between clinics that appear organized and clinics that actually maintain a reliable room-turnover standard. In his view, the challenge is rarely whether staff understand that cleaning matters. The challenge is whether every room reset follows the same disciplined pattern when the pace increases. A room can be cleaned quickly and still miss a key contact area. It can also be cleaned thoroughly one time and unevenly the next. That is why process design matters. Without a repeatable workflow, infection-control quality becomes overly dependent on individual memory, staffing rhythm, and the pressure the shift is under at any given moment.
That observation aligns with what many outpatient managers already know from experience. Variation usually enters through ordinary operational stress rather than an obvious breakdown. A busy waiting room compresses time. A staff transition interrupts continuity. A partially stocked cart changes the order of tasks. A clinical need pulls attention elsewhere. None of these factors is unusual. All of them are common. The point of workflow standardization is to create enough structure that those normal disruptions do not quietly erode the quality of room turnover.
Patient Trust and Audit Readiness Depend on the Same Thing
In urgent care, infection-control consistency is not only a technical concern. It is also a trust concern. Patients may not know the exact cleaning sequence used between visits, but they are highly attuned to signs of order, cleanliness, and professionalism. They notice whether a space feels reset, whether surfaces appear attended to, and whether the environment feels controlled. That perception matters because urgent care relies heavily on confidence. Patients often arrive without an existing long-term relationship with the site. Their impression of the facility forms quickly, and the physical environment shapes it in ways operators cannot afford to dismiss.
At the same time, the internal value of standardized cleaning goes beyond appearance. The CDC’s outpatient infection-prevention guide reinforces the need for defined procedures, staff training, and reliable implementation in outpatient settings, rather than informal assumptions. That makes infection-control consistency relevant to both audit readiness and patient confidence. A clinic that can describe and demonstrate its room-cleaning workflow is in a stronger position than one that relies on broad assurances. In this sense, patient trust and operational defensibility are built on the same foundation. Both depend on having a process that is clear enough to teach, repeat, observe, and verify.
Why This Issue Is Likely to Grow
The importance of infection-control consistency in Baton Rouge urgent care is likely to grow because outpatient care is not becoming simpler. Facilities are dealing with staffing pressure, variable patient flow, rising expectations for efficiency, and a greater need to maintain dependable standards in public-facing clinical spaces. As those pressures continue, the temptation will always be to define success by pace alone. But speed without consistency is fragile. It may work on a good day and unravel on a busy one. A standardized exam-room cleaning workflow offers greater durability. It helps clinics preserve quality while managing volume.
Conclusion
For Baton Rouge urgent care operators, infection control consistency is becoming an increasingly important part of the outpatient operating model. The issue is not whether exam rooms are cleaned at all. It is whether they are cleaned with enough structure and repeatability to hold up under real clinical pressure. That is a facilities question, a patient-trust question, and an infection-prevention question all at once. In a high-volume urgent care setting, the strongest workflow is not the one that merely looks efficient. It is the one that stays consistent when the day stops being easy.